
Vaccination is now the key topic for effective management of the pandemic. There are many important questions to consider, which we will cover in a bulletin shortly.
This short post considers just one aspect, perhaps the most urgent for UK readers: does it make sense to move away from the original vaccination intention of two doses per individual, spaced three weeks apart, and instead seek to cover twice as many people with one dose each? A second dose would be given later, at around 12 weeks.
Simple figures
At first glance, the trial results from the Pfizer and Oxford/AstraZeneca vaccines make the calculations simple (although here we look only at Pfizer for simplicity).
The Pfizer results [1] note an efficacy [2] of 52% after the first dose and 95% after the second dose. However, this first-dose efficacy figure is very likely an underestimate because some of the trial volunteers who exhibited symptoms shortly after the first dose would have had the disease before the vaccination. The Joint Committee on Vaccination and Immunisation (JCVI) [3] suggested an efficacy figure of 74% (instead of 52%) to allow for this effect. Note that this 74% is the lower bound of a plausible range, i.e. it is also likely an underestimate – and therefore, our working below is likely to understate the potential advantage of the one-dose strategy.
We can consider how many cases of COVID-19 are prevented for a given number of doses in a hypothetical example. Let’s assume there are 1,000 doses and 1,000 people. To keep the sums simple, assume that each person would be materially exposed to the coronavirus and have no prior immunity. (This approach works if a smaller proportion are exposed, because we’re just comparing two numbers for relative size.)
Under a two-dose strategy, we can vaccinate 500 people. Of these people, 95% are now safe from severe COVID-19, but 5% are not. So there are likely to be 25 cases of severe COVID-19 among the 500 people vaccinated, as well as all 500 of the unvaccinated group. This gives a total of 525.
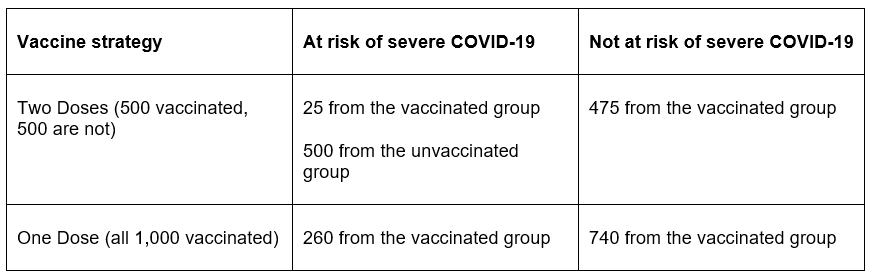
Under a single-dose strategy, we can vaccinate all 1,000 people: 74% (740) are safe from severe COVID-19, the remainder (260) are not.
The substantial advantage to a single-dose strategy is evident – a reduction of cases of around 50% (from comparing 260 against 525). This assumes that the trial efficacy rates hold true in real-life application.
Will these efficacy results translate directly to mortality? The vaccine trial results offer no solid data here, but it is a reasonable assumption to make. We would expect the severity of COVID-19 for a vaccinated person that suffers from it to be no worse than that of an unvaccinated sufferer.
If so, we would reduce the risk of death by the same proportion as above – approximately a halving of mortality.
For brevity, we have not filled this calculation with caveats and confidence intervals. However, one important numerical ‘switch’ made earlier was to replace the one-dose efficacy statistic of 52% with the higher figure of 74%, to allow for COVID-19 cases that were ‘dormant’ at time of injection (noting that 74% was already a bottom-of-range estimate). If we’d used 52% efficacy, the reduction in mortality from a single-dose strategy would be around 10%.
So, looked at simplistically, we expect a material reduction in mortality from pursuing the single-dose approach.
Less simple considerations
Our ‘short and simple’ workings deliberately ignore a range of important considerations:
- How do comparisons translate across the vaccination priority groups? For example, is it as effective to double the number of people vaccinated across the groups, weighing a fully-vaccinated 85-year old against two single-dose 70-year olds?
- What are the implications for each strategy if the vaccine’s efficacy declines materially over time?
- Confusion and concern among people having their second dose appointment postponed.
- The general paucity of data – to some extent regarding numbers of individuals, but more importantly the trials obviously involved relatively short periods.
- The possibility of ‘single-dosers’ providing a particularly fertile environment for the evolution of new vaccine-resistant strains.
We will discuss such considerations in a forthcoming bulletin.
Further information
In addition to information in the references below, we note that the British Society for Immunology has just released a statement regarding the ‘one dose’ strategy, which is broadly supportive of the one dose strategy (conditional on the 12 week follow-up second dose) – www.immunology.org/policy-and-public-affairs/briefings-and-position-statements/COVID-19-vaccine-dosing-schedules.
Endnotes[1] Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine, Polack et al., N Engl J Med 2020; 383:2603-2615 DOI: 10.1056/NEJMoa2034577 – www.nejm.org/doi/full/10.1056/NEJMoa2034577 [2] Efficacy here relates to a comparison of the proportion of the trial populations (vaccinated v placebo) diagnosed with COVID-19: the placebo group comprise 95% of the COVID-19 individuals compared with 5% from the vaccinated group (adjusting for the sizes of the placebo and vaccine groups).[3] https://www.cas.mhra.gov.uk/ViewandAcknowledgment/ViewAttachment.aspx?Attachment_id=103741