
The first two years of the pandemic brought a tragic loss of life, with over 120,000 excess deaths. Almost all of these were a direct result of COVID-19.
Early in 2022 there were fewer deaths than normal for the time of year. The picture worsened as we moved into spring and summer with the Office for National Statistics reporting 15,000 more deaths than average in the last ten weeks. Only a small fraction of these arose during the heatwave.
Excess deaths, typically a niche interest for actuaries and demographers, have made front page news. Speculation is rife as to the underlying causes with suggestions such as ‘lockdown effects feared to be killing more people than COVID’.
With such a large loss of life the desire to point to underlying causes is understandable. We must though take care not to be too simplistic with our explanations. Here we look closer at recent mortality and what can and cannot be inferred from the data available.
Ageing Population
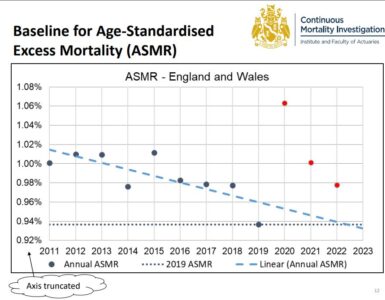
Like many developed countries the UK has an ageing population, so the trend is for deaths to increase. A calculation which simply compares the number of deaths this year to a historical average will overstate excess mortality.
The best way to address this is age-standardisation. This adjusts for changes in population size and age distribution. Taking this approach, the Continuous Mortality Investigation report 10,700 excess deaths in the last ten weeks.
COVID Deaths
There have been around 5,300 deaths with COVID-19 mentioned on the death certificate in the last ten weeks. COVID was the underlying cause for 3,400 of these and may also have contributed to others. Since COVID does not explain all the recent excess we need to look at other causes.
Excess Deaths
One helpful source is the analysis of excess mortality in England provided by the Office for Health Improvement and Disparities (OHID). This allows us to examine deaths by cause, location, and age-group (but currently not combinations of these). Although this is not explicitly age-standardised, allowance has been made to allow for trends.
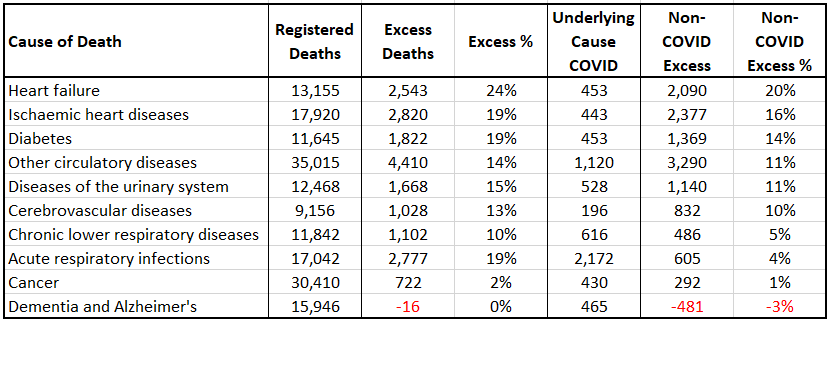
Cardiovascular causes show significant excess mortality. For example, heart disease, heart failure and circulatory diseases. Deaths from diabetes, the urinary system, and respiratory infections are also elevated, though for the latter most of the excess is from COVID. Other significant causes of death, including cancer and dementia, are at or below normal levels.
The table below shows selected causes of death between 11 June and 19 August. More than one cause can be mentioned on the death certificate so these should not be added together.
Root Causes
More work and more granular data are needed to fully understand the underlying drivers of excess deaths not directly caused by COVID. For now, a working hypothesis is some combination of:
1. Elevated cardiovascular risk following COVID infection
A recent article in Nature provides a good summary of concerns around cardiovascular risk, which studies have shown to be elevated for months after a COVID infection. Analysis of international data will be helpful in this regard – if other countries are not seeing elevated cardiovascular mortality this explanation is less plausible. The same logic allows us to discount implausible suggestions such as harm arising from vaccination.
2. Current delays for urgent treatment in the NHS
Waiting times for ambulances and for A&E admission are extremely high. Average ambulance response time for category 2 calls (for example, strokes or heart attacks) was 59 minutes in July, against a target of 18 minutes.
The delays arise from a combination of staff availability (NHS absenteeism has consistently been significantly higher than normal through the pandemic), patient demand (93% of urgent and emergency care beds are occupied), and lack of ability to move patients through the system and discharge them. These are current issues and not, as some have suggested, a consequence of lockdowns in 2020 and early 2021.
3. Missed and delayed diagnoses earlier in the pandemic
The pandemic led to significant disruption to new diagnoses as well as the treatment of chronic conditions. Some appointments had to be cancelled and, in many cases, people chose not to seek treatment. 6.7 million people are now on NHS waiting lists for elective, non-urgent care, up more than 50% since before the pandemic. Additionally, it is estimated that there is a substantial hidden need of people who have not come forward for care. Cancer care is frequently cited as a concern in this regard and, while it clear that this is not currently driving significant excess mortality, it is likely to have a longer-term impact on health and mortality.
Conclusion
A concerning feature of the observed mortality over the last twelve months is the deviation from the usual seasonal pattern seen in the UK. We are no longer experiencing the spikes in deaths of the pre-vaccine pandemic era. Instead, we see death rates consistently at winter levels, leading to excess deaths in the summer months. Despite the record-breaking recent heatwave, NHS pressures and mortality rates seem stuck in a permanent winter. Urgent work is needed to fully understand the root cause of the issues and take steps to resolve them to minimise long-term harm to the nation’s health.
This is an update to a blog written for UK in a Changing Europe.
You can hear Stuart discuss this issue with Tim Harford on a recent edition of BBC More or Less.
Stuart also contributed to a recent BBC Newsnight feature on this topic. There is a clip below and the full episode can be downloaded from iPlayer.